Better Skills, Better Outcomes: Strengthening Bauchi State’s Frontline Capacity for Quality Maternal, Newborn and Child Health Services
Background
Bauchi State faces a persistent burden of high maternal and under-5 mortality rates of ≈1500 deaths per 100,000 live births1 and 153 deaths per 1000 live births, respectively, exceeding the national averages of 512 maternal deaths per 100,000 live births and 132 deaths per 1000 live births, respectively2,3.
EpiC is supporting the government of Bauchi State through its Ministry of Health and State Primary Health Care Development Board (BSPHCDB) to address gaps in maternal, newborn, child health and nutrition (MNCH+N) services by improving access to and the quality of integrated MNCH+N services across 16 priority high-burden LGAs.
To improve the quality of care and close gaps in MNCH+N services, EpiC is strengthening the healthcare system by systematically enhancing healthcare workers’ competencies across the 16 LGAs through 24 mentorship hubs established using a hub-and-spoke model. EpiC is deploying a low-dose high-frequency (LDHF) training strategy through these mentorship hubs. LDHF training is an evidence-based alternative to traditional training models that focuses on concise, targeted, and repeated on-site learning sessions, complemented by ongoing mentorship and supportive supervision.
Hence, EpiC, in collaboration with the State, conducted a 7-day Integrated Refresher Training from April 16–22, 2026. The training workshop brought together key maternal, newborn, and child health (MNCH) stakeholders from the 16 LGAs and State-level MNCH supervisors, including LGA MCH and deputy MCH focal persons, MNCH staff from the Bauchi State Primary Health Care Development Board (BSPHCB), the Bauchi State Health Management Board (HMB), EpiC consultants from the 16 supported LGAs, and Subject matter experts.
The refresher training of trainers (TOT) workshop aimed to strengthen the competencies of the cohort of mentors who would operationalize these mentorship hubs. The mentors will provide mentorship across Basic Emergency Obstetric and Newborn Care (BEmONC/ENCC), Integrated Management of Childhood Illness (IMCI), Quality of Care (QoC), and Maternal and Perinatal Child Death Surveillance and Response (MPCDSR) through the mentorship hubs. The training employed an integrated approach to reinforce the continuum of care while linking clinical skills, quality improvement, and accountability mechanisms.
Training Overview
- Duration: 7 days
- Participants: 80 participants comprising MCH LGA and State level supervisors (midwives, nurses, public health officers, CHEWs, facility managers, and EpiC consultants)
- Coverage: 16 priority LGAs
- Key Training Components:
- BEmONC/ENCC (Days 1–3)
- QoC/ MPCDSR (Day 4)
- IMCI (Days 5–6)
- Quality of Care (Day 7)
Key Learning Areas
- Improved Clinical Competence in Basic Emergency Maternal and Newborn Care (BeMONC &ENCC Services)
Participants updated their knowledge and strengthened skills in managing obstetric and neonatal emergencies, including pre‑eclampsia/eclampsia, neonatal resuscitation, essential newborn care, and postpartum haemorrhage. Didactic lecture discussions updated knowledge, while practical simulations, demonstrations, and return demonstrations reinforced learning and improved confidence and adherence to national protocols.
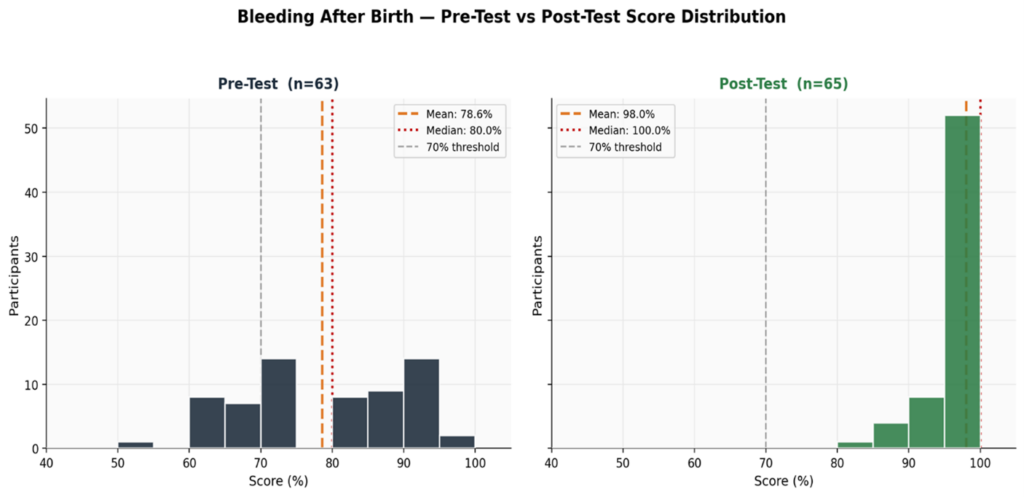
Pre-Eclampsia and Eclampsia: Participant skills were strengthened through didactic lecture discussions, practical hands-on demonstrations, and return demonstrations using case studies. More than half (56.5%) of the participants reported the management of Pre-Eclampsia and Eclampsia as a key learning from the training, while 93.5% reported greater confidence in their Pre-Eclampsia/Eclampsia management skills.